| | | L'avis des experts du Naproxcinod : la polémique enfle |  |
|
+16madrid Virtuelle lazha59 cambl62 Carlos Alonso (carlos-al) gregnorman Olivier Guyonnet(nicoxyd) ncx ARCVOL ristic vinsse beber xocin Benoit Maritan JeanCox Philippe Vaillantpvailla8 20 participants | |
| Auteur | Message |
|---|
Philippe Vaillantpvailla8
Nombre de messages : 1765
Date d'inscription : 13/03/2007
|  Sujet: L'avis des experts du Naproxcinod : la polémique enfle Sujet: L'avis des experts du Naproxcinod : la polémique enfle  Mer 19 Mai - 7:44 Mer 19 Mai - 7:44 | |
|
La polémique est faite autour des publications que pourrait faire Nicox pour montrer les avantages du Naproxcinod au niveau de l'absence d'élévation de la pression artérielle.
La critique de base est donc plus dans la promotion du Naproxcinod que dans la discussion des données soumises à la FDA.
On reproche aux experts de d’aller au-delà de leur compétence et de d’envisager la promotion qui pourrait être faite du Naproxcinod autour des articles déjà parus dans les grandes revues. L’un d’eux explique même que ne pas donner de label au Naproxcinod serait pire car la promotion ne reposerait uniquement que sur les publications du Naproxcinod.
La polémique tourne donc autour de la promotion des produits pharmaceutiques et le marketing de certains laboratoires. Nicox fait les frais de cette polémique alors qu’il n’a jamais commercialisé de produit et que l’on peut difficilement lui reprocher de telles pratiques. Le rôle des experts n’est pas de prévoir le marketing des laboratoires.
Nicox a réussi à faire naître la polémique, donc une grande publicité autour des réserves des experts.
La discussion des leaders d’opinion médicale, des laboratoires qui vont se sentir visés, de la FDA qui voit le champ de discussion des experts se déplacer sur un terrain qui n’est pas le leur ne peut qu’être profitable à Nicox. La non approbation du label du Naproxcinod fait beaucoup de bruit sur la base des critères qui ont été choisis.
Les experts du camp de Nicox vont avoir beau jeu d’exploiter cette faiblesse des bases des critères de jugement. Des experts de pointe en pathologie cardio-vasculaire jouent leur réputation en ayant défendu le Naproxcinod. Les leaders de cardiologie des comités de lecture ou des congrès (les plus important du monde) sont mises en cause dans l’acceptation du publications de données et de conclusions que les experts de des comités mettent en doute. L’éthique des plus grands leaders d’opinion médicale est indirectement mise en doute lorsque l’on conteste les données et l’interprétation des résultats des articles parues dans les plus grandes revues du monde mondical.
Les laboratoires peuvent y voir une attaque en règle contre leur pratique de marketing. Les plus grands laboratoires ne pourront laisser passer une telle polémique sans réagir (même si se sont des potentiels concurrents du Naproxcinod). Le doute que cela induit sur leur probité et sur les critères qui pourraient naître pour les prochaines mises sur le marché pour leurs propres molécules ne peuvent être acceptés.
L’avis des experts des comités est déjà dans la presse à scandale médical…Une belle publicité pour le Naproxcinod si la FDA l’accepte à la commercialisation.
| |
| | | | JeanCox

Nombre de messages : 1008
Age : 70
Date d'inscription : 19/12/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 7:48 | |
| Merci beaucoup Philippe pour ce post d'analyse comportementale qui va bien au-delà des premières réactions épidermiques suscitées par le refus des experts.  C'est un post à lire et a relire, et à faire parvenir au staff de NicOx (si ce n'est déjà fait ?) | |
| | | | Benoit Maritan

Nombre de messages : 432
Age : 48
Localisation : Nouméa
Date d'inscription : 01/09/2008
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 7:51 | |
| - Philippe Vaillantpvailla8 a écrit:
- La polémique tourne donc autour de la promotion des produits pharmaceutiques et le marketing de certains laboratoires. Nicox fait les frais de cette polémique alors qu’il n’a jamais commercialisé de produit et que l’on peut difficilement lui reprocher de telles pratiques. Le rôle des experts n’est pas de prévoir le marketing des laboratoires.
Sauf que Nicox a voulu faire bcp de bruit avec le pré-marketing et que les experts l'ont visiblement mal vécu!
C'est un peu l'arroseur arrosé! | |
| | | | Philippe Vaillantpvailla8
Nombre de messages : 1765
Date d'inscription : 13/03/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 8:17 | |
| Le pré marketing est trèsimportant. C'est la pratique habituelle des laboratoires. Certains experts sont visiblement en guerre contre les laboratoires. Le refus de l'approbabtion risque d'être discrédité car ne reposant pas sur les critères que la FDA leur a fixé.
Les comités sont bien partis pour se faire aligner les laboratoires, les leaders d'opinion médical, la FDA...Les actionnaires ne peuvent que s'en féliciter. Le pré marketing des comités de rhumatologie et des facteurs de risques des médicaments est excellent. Les médecins vont tous entendre parler du Naproxcinod, les patients vont même en entendre parler...C'est inespéré pour les ventes "over thecounter" si le Naproxcinod est commercialisé avec une belle phaseIV. | |
| | | | xocin
Nombre de messages : 18
Age : 51
Localisation : Rennes
Date d'inscription : 11/06/2008
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 8:24 | |
| Attention attention amis CoXiens je sens poindre un regain de folie depuis hier suite à cette polémique. Vous oubliez trôp vite la douche froide que nous venons de subir, rien n'est joué loin de là !! Mais bon cela fait du bien de voir que ça n'est pas fini et que Cox n'est pas n'a pas abattue sa dernière carte ....
Forza NiCox | |
| | | | Philippe Vaillantpvailla8
Nombre de messages : 1765
Date d'inscription : 13/03/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 8:25 | |
| Tu as raison JeanCox, il faut prévenir Nicox que le Naproxcinod va être en rupture de stock dés la première semaine de mise sur le marché...
"3 blessés de 70 ans au drugstore. Le Naproxcinod mis en cause. La denière boite était très convoitée." | |
| | | | beber
Nombre de messages : 685
Date d'inscription : 25/11/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 8:27 | |
| Philippe tu navigues dans les milieux dans lesquels tu situes ton scénario (FDA, labos, "leaders médicaux" américains...), ou c'est juste un roman ?
Je précise que je ne critique pas ton post, je cherche à l'évaluer. | |
| | | | Invité
Invité
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 8:28 | |
| attention, vous emballez pas ... |
| | | | JeanCox
Nombre de messages : 1008
Age : 70
Date d'inscription : 19/12/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 8:31 | |
| - xocin a écrit:
- Attention attention amis CoXiens je sens poindre un regain de folie depuis hier suite à cette polémique. Forza NiCox
YES  Soyons fous, après tout ne le sommes nous pas depuis très très longtemps ??? Soyons fous, après tout ne le sommes nous pas depuis très très longtemps ??? Et mon proverbe à moi : délire du matin et la journée commence bien ! | |
| | | | vinsse

Nombre de messages : 515
Date d'inscription : 15/05/2008
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 8:33 | |
| http://cme.medscape.com/viewarticle/720992_transcript et c'est des vrais experts ...la porte reste ouverte ....à mon humble avis Blood pressure destabilization is a real concern for some patients who rely on nonsteroidal anti-inflammatory drugs (NSAIDs)/COX-2 inhibitors for pain control, but it's not always easy to know how much of an increase in blood pressure signals a clinically relevant risk. Moreover, adding another antihypertensive agent or discontinuing the NSAID may not be optimal solutions. A new class of anti-inflammatory agents may offer a way to provide adequate pain control without increasing blood pressure. George L. Bakris, MD:
Hello. I am Dr. George Bakris, Professor of Medicine and Director of the
Hypertensive Diseases Unit at the University of Chicago Pritzker School
of Medicine. I would like to welcome you to this CME Spotlight
entitled: "Treating Pain and Inflammation in Osteoarthritis Without
Increasing Blood Pressure."
I am joined by Dr. Carman Ciervo,
Associate Professor and Chairman, Department of Family Medicine,
University of Medicine and Dentistry of New Jersey School of Osteopathic
Medicine, Stratford, New Jersey; and Dr. William White, Professor and
Chief, Division of Hypertension and Clinical Pharmacology, Pat and Jim
Calhoun Cardiology Center, University of Connecticut School of Medicine,
Farmington, Connecticut.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 1.
(Enlarge
Slide) |
There are 3 goals of this
activity: first, to assess the risk for blood pressure (BP)
destabilization in patients taking nonsteroidal anti-inflammatory drugs
(NSAIDs) or COX-2 inhibitors; second, to summarize the role of nitric
oxide (NO) in hypertension and arthritis; and third, to evaluate the
potential role of a new class of NSAIDs that does not cause increases in
BP.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 2.
(Enlarge
Slide) |
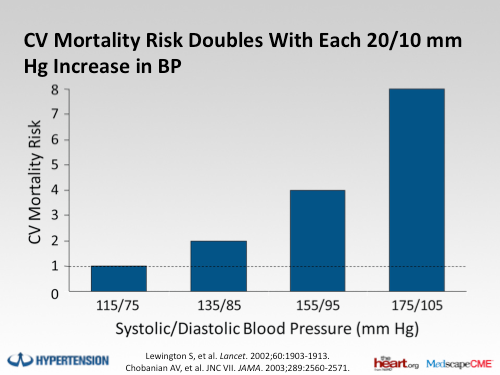
Before we start, it is important
to have a little background in terms of the information that physicians
should have at hand. About 29.4 million people in the United States have
osteoarthritis (OA), and about 15.9 million people with OA also have
hypertension. NSAIDs and COX-2 inhibitors can cause increases in BP and
interfere with the management of hypertension. Even small increases in
BP can be associated with significant increases in cardiovascular risk
in the general population.
Today, we will be discussing the
clinical significance of the effects that NSAIDs have on BP, some of the
underlying mechanisms, particularly the role of NO, and the development
of a new class of anti-inflammatory agents that does not have an
adverse effect on BP.
Carman, let's start by asking a
few questions. First, how often do NSAIDs cause a problem with BP?
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 3.
(Enlarge
Slide) |
Carman A. Ciervo, DO: I
actually think this can be broken down into 2 questions, and these are:
how often does it cause a problem, and how often is that problem
recognized?
Certainly, when patients are
coming into a busy primary care office, something as small as a 2-3 mm
Hg increase in systolic BP may not be recognized initially by the
clinician. However, over a period of time, looking at BP and recognizing
the importance of controlling even small increments of BP, it is my
hope that this would be addressed.
Dr. Bakris: Okay. How
often do you think clinicians need to change BP medications in people
taking NSAIDs?
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 4.
(Enlarge
Slide) |
Dr. Ciervo: Again, in the
primary care arena, this is a very important question, because not only
are patients coming to us for multifactorial diseases, including their
high BP, their hypercholesterolemia, and very often their OA, as well as
other disease processes, they are seeing other clinicians, and these
clinicians are making adjustments to their medication profile for
various reasons.
When they come to us, and we see
an increase in BP, very often, the initial reaction is to increase the
medication that they are on and maximizing BP control with a single
agent if possible, but this may also require adding another agent to
control BP. When you think about how often this occurs, it is a fair
amount of time considering that a lot of what a primary care physician
is seeing is related to control of BP along with its comorbidities.
Dr. Bakris: Now, you made
a comment, and I just want to come back to it. You were talking about
increases in BP of 2-4 or 5 mm Hg, but how much of an increase are you
really concerned about? I mean, the patients came in, they were hurried,
and maybe they were at 132 mm Hg [systolic]. Now you have checked them
out, and they are at 136 mm Hg -- they are still below 140 mm Hg. What
is the big deal? How much of a difference in BP are you going to need to
really alert you that you better do something?
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 5.
(Enlarge
Slide) |
Dr. Ciervo: It is my hope
that my colleagues would recognize that even a small increase in BP (2
mm Hg) can have an effect on cardiovascular morbidity and mortality. In
reality, your point is very well taken: very often, it is more of the
norm to say, "Well, let's see what we can do as far as rechecking your
BP, and we will bring you back in a couple weeks, or we will see what it
is at the next visit." In reality, the BP really should be addressed at
each and every visit, and small increments of BP are being recognized
as very important in looking at and making a change as needed.
William B. White, MD:
Part of this question is the limits of detection of the observer -- that
is us, the doctors.
Dr. Bakris: Right.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 6.
(Enlarge
Slide) |
Dr. White: When you learn
from a population study or a meta-analysis of trials that NSAIDs raise
BP by 5 mm Hg or 6 mm Hg -- and some do and some don't, of course --
that is a population mean, and some people have no change in BP, though
some have much larger changes. In terms of an individual patient, you
are not likely to pay attention to or be able to detect a 2 mm Hg or 4
mm Hg difference in pressure; that would be very unlikely, because of
the inherent variability. So you probably are going to be looking in
terms of, "Well, you are about 5 or 10 mm Hg higher than last time, or
10 or 20 mm Hg higher, why is that?" Then, an intervention is going to
be considered. NSAIDs are not going to always be first on the list as to
what caused that problem in the first place.
Dr. Bakris: Right. Bill,
you raise a very important point: 2, 3, and 4 mm Hg are within the
standard error, if you will, of the measurement. It is important to
understand that a lot of patients, especially elderly patients (those
over 65 years), and even obese patients who eat a lot of salt can have
up to 10-15 mm Hg increases; those would pull the trigger. But I wanted
to get back to the point about prehypertensive patients who now are
becoming hypertensive. If your systolic BP is 132 mm Hg or 134 mm Hg,
your pressures have been well controlled, and now all of a sudden, you
are at 142 mm Hg or 140 mm Hg, but you rushed in, and you were late for
the appointment: How likely do you think the physician is to recheck the
BP after you have actually calmed down and waited a while? Some offices
do; some offices don't. Of course, patients do not want more medicine;
they certainly don't want an increase in medicine. So they are going to
say, "Wait a minute, wait, I rushed in here." What do you think is going
to happen, Carman, in that setting? Do you think physicians are going
to recheck it? Should they recheck it? Should they be asking about other
causes?
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 7.
(Enlarge
Slide) |
Dr. Ciervo: Again,
ideally, you would want the physician to have that opportunity to let
the patients sit down, collect themselves, and recheck the BP in 10
minutes, and see whether that 142 mm Hg comes down to 132 mm Hg. If, in
fact, it doesn't, it is very important to assess what the cause is for
that increase in BP. It's important to say, "Listen, we need to bring
your BP under control, and we need to make a change." It is also
important to recognize that very often, these patients are
self-medicating, and there are numerous over-the-counter NSAIDs that
these patients are on. Unless the physician is astute enough to ask
them, "What other medications are you taking over the counter?" [this
information will be missed]. It is surprising. Every time I see a
patient, I ask, "What other medications are you taking, both
complementary and alternative medicines, and over-the-counters?" It is
not all that infrequent that the patient talks about naproxen or
ibuprofen, and not just a little bit of it, but a significant amount.
Patients are savvy enough to know that they can take multiple
over-the-counter medications to equal [the dosage that is in] a
prescription medication.
Dr. Bakris: Right, and
that is a good point. Just as a point of reference to physicians:
usually, the over-the-counter medications that are sold are 50% of the
prescription strength. Savvy patients just double the medications, and
then life is good, or, as you say, they take multiple different NSAIDs
and get the same effect. It is an important point. Well, Carman, thank
you very much. We are going to discuss this a little bit later in the
program.
I want to turn now to Billy White
to explain how NSAIDs increase BP from a pathophysiological
perspective. What are the subtypes of patients at risk? What are the
mechanisms that deal with NO and other mechanisms for this increase?
What is really going on?
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 8.
(Enlarge
Slide) |
Dr. White: It is actually
pretty complicated. There is this very complex cascade of events where
NSAIDs interfere with the transition of arachidonic acid to form
prostaglandins. Some of the prostaglandins are associated with
inflammation, so thereby, you get pretty good anti-inflammatory effects
when these medications are administered, and they differentiate
primarily by their half-life and strength and so forth. Generally
speaking, from the patient's perspective, pain relief is pain relief. So
they are not much different in that regard.
Some of the patients who take
NSAIDs get absolutely no hypertensive responses. They have excellent
renal function; they don't take BP drugs; their kidneys respond
beautifully to producing more prostaglandins per nephron to take over
for whatever was removed by the NSAID, so they don't have a problem.
That is probably 80% of the people who take these drugs.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 9.
(Enlarge
Slide) |
However, we don't see those
people as specialists in hypertension or nephrologists. We see the
people who get into trouble, and those are individuals who have
underlying renal disease, a history of heart disease, or they are taking
medications that make them salt-sensitive by definition. Primarily,
they are renin-angiotensin blocking drugs, and to some extent these are
the diuretics and the beta-blockers.
In that group, there are 2 things
going on: prostaglandin E is a very important mediator of salt and
water balance. If you get rid of it by an NSAID, all of a sudden, your
ability to have a normal natriuresis is declined; it is by 40% in the
second day of taking an NSAID. If you are eating your typical amount of
salt, it is not getting out of there, so volume goes up.
Many individuals can get rid of
that and become homeostatic at the expense of a little rise in BP -- not
much, 1 mm of mercury -- so they are okay, too. Others can't do that;
they have got to go up 3-10 mm Hg in order to maintain homeostasis of
renal function and blood flow within the kidney.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 10.
(Enlarge
Slide) |
This is the kind of person you
will see coming into your office: those who have edema, newly developed
destabilized BP, and maybe even congestive heart failure symptomatology.
Lastly, some drugs and some
conditions, including renal disease, diabetes, etc, deplete the system
of prostacyclins, making NO the kind of background modifier of good
blood flow. Therefore, you have to be careful about whether this will be
affected negatively in any way when you take out too much of the
prostaglandins. Some antihypertensive drugs have a pretty good effect on
NO, and some don't. We have to look at that in a very complicated way,
unfortunately, to decipher it. But the bottom line for the practicing
doctor is that drugs that interfere with blood flow, the prostaglandin
blockers such as NSAIDs, and those that increase salt and water
homeostasis, make your patient more likely to become hypertensive.
Dr. Bakris: Now, those
are good points, and before we go on to the next topic, I want to focus
on something you said. You said some antihypertensive drugs have better
effects than others. It is well known that calcium antagonists actually
[attenuate] some of this BP-raising effect that is seen with NSAIDs, but
really, other classes of drugs don't like the renin-angiotensin system
blockers, and even diuretics, don't really have that effect. What is
going on with that?
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 11.
(Enlarge
Slide) |
Dr. White: We learned a
long time ago that in low-sodium balanced states, drugs that affected
angiotensin removal worked really well. You load up the body with
sodium, and they just don't seem to have the same benefit; they can't
counteract it. So then, you add a diuretic, and they work great again.
The calcium antagonists seem to be somewhat impervious to salt intake.
They may work a little less well in a person who is taking 12 gm of
salt/day compared with 2 gm, but it is just not as dramatic, because
they are working ubiquitously on the vasculature as a smooth muscle
vasodilator. A lot of physicians give calcium channel blockers to people
who are "saltaholics," knowing that at least that drug probably is
going to work, although it may not be the only thing that is necessary.
It is the same way with NSAIDs: if you have got somebody who takes
high-dose NSAIDs who also likes to eat salt, it is a double whammy
against an angiotensin-converting enzyme inhibitor or an angiotensin
receptor blocker working properly.
Dr. Bakris: Right.
Dr. White: But if they
are on a calcium channel blocker, they are most likely going to be okay.
[This is probably also true for] the alpha blockers, not that we use
them as much as a primary drug in hypertension; they seem to be sort of
less likely to be attenuated by NSAIDs compared with renin-angiotensin
system inhibitors.
Dr. Bakris: That is a
good point. I want to move to this whole new area of the COX-inhibiting
nitric oxide donators (CINODs) and the merging pharmacology of this
compound married to NSAIDs. What can you tell us about this?
Dr. White: Theoretically
in the lab, a number of years ago, somebody realized that if you have
some disease entity, whether it is diabetes, nephrosclerosis, or
hypertension that is leading to a loss of general homeostatic
prostacyclin in the renal vascular bed, then what is left to help renal
blood flow?
Dr. Bakris: Right.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 12.
(Enlarge
Slide) |
Dr. White: That would be
NO. So could there be a way to enhance NO delivery to sort of fight what
is going on when NSAIDs are used? These clever chemists came up with a
way of linking NO molecules by an ester link to a standard NSAID, in
this case, naproxen, with the cyclooxygenase NO-donating moiety. This
new agent is called it naproxcinod. What happens is that the drug has
the same amount of naproxen as what is available now, but when the drug
is ingested and it gets into the cell, an esterase cleaves the ester and
breaks off the NO molecule, so it gets into the cell, and it causes
vasodilation. It does this over a few hours; it is not as fleeting as it
would be if it was just located in the circulation. It mitigates some
of the BP increase that would be seen as a result of the prostacyclin
blockade.
Dr. Bakris: So it
attenuates the increase.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 13.
(Enlarge
Slide) |
Dr. White: It attenuates
the increase. It doesn't lower the pressure by itself; it is not a
BP-lowering drug by itself. It is not an antihypertensive drug.
Dr. Bakris: Right. It
shouldn't be confused with a nitrate, for example.
Dr. White: Exactly. It is
not a nitrate; it is not an organic nitrate, in fact, it works
differently; it works intracellularly. These agents don't seem to
develop tolerance at all. I don't think there is any venodilation with
NO by itself as there would be with organic nitrates. So it is very
different in its transfer into the cell and in the way it is moving
hemodynamically.
Dr. Bakris: Are there any
comparative studies with naproxen by itself or the naproxcinod vs
naproxen on BP? Theoretically, this is all very nice, but do we have any
patient data that would help guide us in any direction in terms of BP
changes?
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 14.
(Enlarge
Slide) |
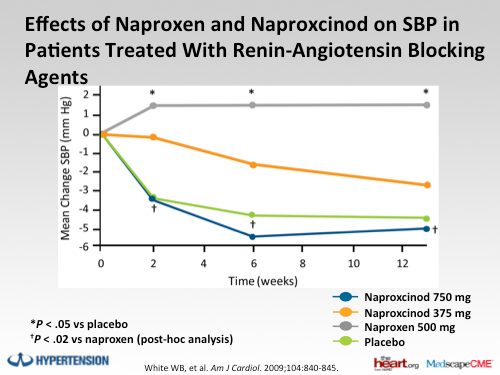
Dr. White: There have
been some very well-done ambulatory BP studies that have examined the
changes on naproxen vs naproxcinod, and there is also one that actually
has ibuprofen in the mix, too. The general finding from that is that
naproxcinod does not raise BP to the same extent that naproxen does; it
is about 2-5 mm Hg lower over the whole 24-hour average time period in
comparison, and it is about 3.5 or 3.8 mm Hg less than ibuprofen. These
are the kind of changes that indicate that it is basically acting a
little bit like a placebo, even though we did not have a placebo in
those studies.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 15.
(Enlarge
Slide) |
Dr. Bakris: That is very
nice to know, but [Dr. Ciervo], is that a big deal? If you have patients
who are older and are taking NSAIDs for OA or whatever pain conditions
they have, and you see that these patients are having BP issues, you
need to adjust their BP medicines to take care of their BP issues. How
likely would you be, if this drug was available to you, to recommend it
to the patient?
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 16.
(Enlarge
Slide) |
Dr. Ciervo: Considering
the multitude of disease processes that you have to address in a
relatively short period of time in the primary care setting, it is
definitely something that I would consider. The fact that I can use a
product that is not going to destabilize the BP, and would still provide
the relief that, for example, in this case, naproxen would provide, is
very important to me because then I don't have to focus on the
destabilized BP. In that same office visit, I may be addressing their
diabetes, their hypercholesterolemia, and anxiety disorder that they are
coming in with. [The benefits are that I would] have a product that is
not going to force me to be concerned about modification of BP
medications and the associated cost of changing the medication, and then
the inconvenience of bringing the patient back in and the cost of
bringing the patient back in. Very often, these patients are coming in
with a caretaker, but even if they are coming in by themselves, there
are still associated costs that patients are quite aware of today.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 17.
(Enlarge
Slide) |
Dr. Bakris: Let's not
forget about side effects, because it is well known that for most
classes of antihypertensive drugs, as you are increasing the dose, the
number of side effects increases. We talked earlier about calcium
antagonists, which are well known to have higher edema rates, especially
in women (some women really abhor the fact that they can't wear their
shoes, but their BP is okay). That is an important issue. With
diuretics, if you increase the dose, you are more likely to have
metabolic side effects as well as potassium issues. So that does have to
be brought into play. How likely is it that patients will be receptive
to this new drug if they don't have to adjust their BP medications and
are less likely to take more pills?
Dr. Ciervo: Let's just
say this: there aren't too many visits where the patient says, "You are
adding another medication? That is great."
Dr. Bakris: [laughter]
That is right.
Dr. Ciervo: You could
take almost a small educational vignette and tell the patient, "Listen,
we are going to be able to provide you with something that is going to
control the pain [without increasing your BP], because it is important
to control BP." We recognize that as physicians, but if the patient has a
choice between being able to be ambulatory and perform their activities
of daily living and having their BP go up [vs not having adequate pain
control], they are still going to use the NSAID. Even if I am not
prescribing that NSAID, they are still going to use it if they have to
get it over the counter, so that they can remain functional, because
that is what is important to them -- that and pain control.
Dr. Bakris: Very good.
Dr. Ciervo: So the fact
that I could educate them and tell them, "We can use a product that is
not going to increase your BP," would increase compliance without me as
the physician having to worry about those increases in BP that are going
to occur.
Dr. Bakris: Right. Billy,
any final quick thoughts?
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 18.
(Enlarge
Slide) |
Dr. White: The other
aspect of this is that there is a very large number of people who we
have in our wisdom called prehypertensives or borderline hypertensives
in the United States who also could have OA. The studies that we have
done at this point in time demonstrate that the chances of making a
prehypertensive patient become a sustained hypertensive patient on a
conventional NSAID are pretty high. It is about 20%-25% because they are
going to cross that line of 5 or 6 extra mm, and that, in fact, is cut
in half when you give an NO-donating naproxen. So that will be a
targeted population, if you will, to consider for this drug.
| [ CLOSE
WINDOW ]
<blockquote>
 </blockquote> </blockquote>
Slide 19.
(Enlarge
Slide) |
Dr. Bakris: Let me summarize for you what we have said: NSAIDs are well known to diminish BP control in hypertensive patients as well as transform a subgroup of prehypertensive patients to actually having hypertension. Small increases in BP are known to increase cardiovascular risk in the general population. Physicians should be aware of these facts and assess BP in the subgroup of patients who are most likely to have these changes and respond appropriately. Carman, Billy, thank you very much for joining us today. | |
| | | | Philippe Vaillantpvailla8
Nombre de messages : 1765
Date d'inscription : 13/03/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 8:39 | |
| Le marketing est basé sur le fait que l'on parle du produit.
Les experts sont en train de bâtir une image du Naproxcinod :
"un médicament enthousiasmant".
"une non approbation basé sur de mauvais critères"
"des articles majeurs pourraient influencer les ventes du Naproxcinod"
"il est préférable de donner une notice pour limiter l'impact des articles"
« Non au Naproxcinod pour contrer le lobbying de la pharmacie »
Cela devrait faire réagir de tous les cotés avec amplification, déformation, attractivité du produit renforcée...
Dernière édition par Philippe Vaillantpvailla8 le Mer 19 Mai - 10:50, édité 1 fois | |
| | | | JeanCox
Nombre de messages : 1008
Age : 70
Date d'inscription : 19/12/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 8:45 | |
| Merci Vincent, certaines évidences sont bonnes à rappeler  | |
| | | | ristic

Nombre de messages : 124
Age : 76
Localisation : FOURAS 17
Date d'inscription : 07/09/2008
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 10:04 | |
| Puisque Sophia n'est pas bien de Cannes, je vous fais la présentation du film de ce jour " La Saga du Napro" scénario de Philippe Vaillant Metteur en scène Michele Garuffi Acteurs principaux : FDA - Merck - B&L - Ferrer - Pfizer et les Experts Figurants : Petits Porteurs En touscas merci Philippe pour ce post qui donne un nouvel éclairage pour la suite | |
| | | | ARCVOL
Nombre de messages : 75
Date d'inscription : 11/06/2008
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Mer 19 Mai - 10:44 | |
| +1 pour l'humour le moral revient au beau fixe comme le printemps. Petite satisfaction qui compense pas les pertes des investisseurs LT ce sont a priori les day trader qui se font pas mal plumer en ce moment. | |
| | | | Philippe Vaillantpvailla8
Nombre de messages : 1765
Date d'inscription : 13/03/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Ven 21 Mai - 23:08 | |
| Les experts ont voté avec leur pieds...
Certains ont voulu réduire le potentiel commercial du Naproxcinod et se rendent compte que le marketing sans notice pour le Naproxcinod peut être plus porteur...Mais pourquoi pensent-ils que le Naproxcinod va être commercialisé??? | |
| | | | ncx
Nombre de messages : 94
Date d'inscription : 15/03/2010
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 12:16 | |
| - Philippe Vaillantpvailla8 a écrit:
- Le pré marketing est très important. C'est la pratique habituelle des laboratoires.
Si on en croit le Lancet, c'est pas si habituel car ils ont écrit un article concernant le Naproxcinod et une pratique un peu douteuse : - Citation :
- The Lancet, Volume 375, Issue 9712, Page 347, 30 January 2010
This policy seems problematic when it concerns a supplement that contains an Introduction (which misleadingly states that “the articles…represent the current state of the art in the pharmacological management of OA [osteoarthritis]”), together with three articles, two of which are dedicated largely to the subject of nitric oxide in inflammation and naproxcinod as an “attractive alternative” to existing therapies. It is even more problematic when naproxcinod is undergoing FDA review at the same time as the publication and wide distribution of this non-peer-reviewed supplement.
Some may argue that supplements and custom publications are routinely thrown away, so why worry. But the deliberate effort to subvert peer-review at a delicate time for an as yet unlicensed product should be a cause for concern. Others may say that this kind of publication is no worse than display advertising. Except that a display advertisement can only be for a licensed product, which naproxcinod is not. - Philippe Vaillantpvailla8 a écrit:
Les médecins vont tous entendre parler du Naproxcinod, les patients vont même en entendre parler...C'est inespéré pour les ventes "over thecounter" si le Naproxcinod est commercialisé avec une belle phaseIV. Je doute que le terme "inespéré" soit le plus approprié... - Philippe Vaillantpvailla8 a écrit:
Les experts ont voté avec leur pieds...
Certains ont voulu réduire le potentiel commercial du Naproxcinod et se rendent compte que le marketing sans notice pour le Naproxcinod peut être plus porteur... Ah ben finalement c'est une bonne chose qu'on ait essuyé un refus, ouf ! Au fait, ok les experts de l'AC sont des incompétents, mais quid de la FDA ? Il y a eu méprise sur le dossier et ont confondu avec un anti-HTA ? Impossible puisque NicOx nous a assuré que ça se passait bien et qu'il y avait des discussions régulières pour monter un dossier bien ficelé. Du coup se tromper d'objectif thérapeutique est difficilement compréhensible. Puisque l'AC a tort et que la FDA devrait valider, autant revenir au document initial émis par cette dernière : http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ArthritisDrugsAdvisoryCommittee/UCM211466.pdf - Citation :
- Indication
The Applicant seeks an indication of, “for the relief of signs and symptoms of osteoarthritis.”
[...]
The issues related to the BP effect of naproxcinod to be addressed are as follows:
• Related to efficacy:
o Presence of an antihypertensive effect (not applicable since the product was not developed for this indication and the response was not superior to placebo) Et il serait bon que tous les points soulevés par la FDA (et non l'AC) déjà évoqués ici trouvent une réponse si on veut une approbation. | |
| | | | Philippe Vaillantpvailla8
Nombre de messages : 1765
Date d'inscription : 13/03/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 12:49 | |
| Les tirets à part d'article dans de grande revue sont de pratique courante et efficace en terme de promotion. C'est peut être cette efficacité qui agace les experts des commissions.
Les ventes "over the counter" n'étaient pas visées clairement par Nicox. La discussion, la polémique d'un produit en fait la promotion indirectement, encore faut-il que le produit soit commercialisé.
La FDA n'a pas donné de méthodologie pour évaluer le Naproxcinod pour les experts des commissions. L'absence ou lamoindre élévation de la pression artérielle du Naproxcinod ne peut pas être évalué comme l'association du Naproxène et d'un antiHTA.
la FDA doit aussi préciser les critères d'évalution de cet effet secondaire des AINS et de cette absence ou moindre effet d'élévation de lapression artérielle du Naproxcinod. | |
| | | | Olivier Guyonnet(nicoxyd)
Admin

Nombre de messages : 2361
Age : 66
Localisation : Seine et Marne (77)
Date d'inscription : 03/02/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 13:20 | |
| - Philippe Vaillantpvailla8 a écrit:
La FDA n'a pas donné de méthodologie pour évaluer le Naproxcinod pour les experts des commissions. L'absence ou lamoindre élévation de la pression artérielle du Naproxcinod ne peut pas être évalué comme l'association du Naproxène et d'un antiHTA.
la FDA doit aussi préciser les critères d'évalution de cet effet secondaire des AINS et de cette absence ou moindre effet d'élévation de lapression artérielle du Naproxcinod. C'est bien là que le bât blesse, côté FDA: quand les experts demandent au représentant de la FDA quels critères doivent être retenus dans les études cliniques, et que celui-ci leur retourne la question, on croit rêver... Je ne suis pas "bisounours". Je sais que nous sommes entourés de requins, et que NicOx a sans doute pêché par une trop grande confiance dans le respect des procédures et réglementations. La politique s'est mêlée aux débats des experts, et leurs réflexions ont démontré qu'ils étaient plus souvent dans la réaction épidermique subjective que dans le point de vue scientifique objectif. Le fait qu'ils soient choisis sur un critère de non collaboration avec les labos conduit à ne pas avoir le meilleur panel d'experts du sujet (qui étaient dans l'équipe de promotion du napro...), et d'y compter des pourfendeurs des pratiques de commercialisation des labos. NicOx en a clairement fait les frais. Le fait que ce débat ait été public est toutefois précieux. Il est clairement apparu à beaucoup qu'il avait été mal conduit et manquait de rigueur scientifique, voire de rigueur tout court. La presse anglo-saxonne s'en est fait l'écho, tandis que notre presse franchouillarde s'est complue - comme d'habitude - dans le sensationnel et la critique du "made in France". A cet égard, je n'évoquerai la saillie de Mme Wapler que pour souligner sa méconnaissance du dossier: affirmer que le NO porté par le napro disparaît en quelques dizièmes de secondes dans l'estomac dès l'ingestion, et n'aurait donc aucun effet possible sur la durée, prouve à tout lecteur un tant soit peu averti qu'elle ne s'est pas penchée sur l'aspect technologique du sujet... tout cet étalage d'approximations et d'incompétence dans le camp des pourfendeurs du napro est finalement un bon point pour la défense de NicOx. Je ne porterai donc pas le feu dans la maison NicOx, contrairement à ce que certains aimeraient me voir faire. Je demeure confiant dans l'équipe dirigeante et dans le produit. J'observe d'ailleurs que le Conseil d'Administration, qui comprend des personnes éminentes, bien plus qualifiées que moi en développement/marketing de produits pharmaceutiques et en gestion d'entreprise, a maintenu Michele à son poste. Notre intérêt va dans le sens d'un soutien de l'équipe en place dans son combat, car son succès déterminera le nôtre. Je ne serai pas de ceux qui se tirent une balle dans le pied par dépit... Pour autant, je ne méconnais pas les risques: le chemin demeure semé d'épines, et nous tremblerons jusqu'à la décision de la FDA. | |
| | | | gregnorman
Nombre de messages : 440
Age : 64
Localisation : 92
Date d'inscription : 02/06/2008
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 17:00 | |
| - Olivier Guyonnet(nicoxyd) a écrit:
Je ne porterai donc pas le feu dans la maison NicOx, contrairement à ce que certains aimeraient me voir faire. Je demeure confiant dans l'équipe dirigeante et dans le produit. J'observe d'ailleurs que le Conseil d'Administration, qui comprend des personnes éminentes, bien plus qualifiées que moi en développement/marketing de produits pharmaceutiques et en gestion d'entreprise, a maintenu Michele à son poste. Notre intérêt va dans le sens d'un soutien de l'équipe en place dans son combat, car son succès déterminera le nôtre. Je ne serai pas de ceux qui se tirent une balle dans le pied par dépit...
Il n'a jamais été question de se tirer une balle dans le pied, mais de faire preuve seulement d'un peu plus d'esprit critique et de lucidité. Désolé Olivier, mais si nous faisons le bilan de ces 2 ou 3 dernières années c'est zéro pointé sur toute la ligne (à l'exception de l'accord avec B et L et encore, MG n'en voulait pas). J'ai investit dans Nicox pour valoriser mon patrimoine et parce que le projet semblait sympa et attrayant, pas pour que l'on m'explique in fine pourquoi cela n'a pas marché etc.... J'attends donc des dirigeants qu'ils soient professionnels et qu'ils prennent les mesures nécessaires au succés (partenariat, lobbying politique etc.......). Pas qu'ils me tondent à longueur d'AK. Si cela doit passer par l'esprit d'équipe, l'excellence technique où je ne sais quoi, je dirai trivialement que je m'en contre fout et que je n'attends qu'une chose : des résultats tangibles. Pour le moment et cela dure maintenant depuis un moment, les résultats ne sont pas au rendez vous, ne t'en déplaise. Les promesses par contre sont bien toujours au rendez vous. Oui je sais Olivier tu ne trouveras pas mes propos et ma position politiquement correcte. C'est néanmoins celle que je défends et il apparaît que je ne suis pas le seul dans ce cas. | |
| | | | Carlos Alonso (carlos-al)

Nombre de messages : 624
Age : 62
Localisation : Angoulême 16
Date d'inscription : 05/02/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 20:28 | |
| - gregnorman a écrit:
- [>Désolé Olivier, mais si nous faisons le bilan de ces 2 ou 3 dernières années c'est zéro pointé sur toute la ligne (à l'exception de l'accord avec B et L et encore, MG n'en voulait pas).
J'ai investit dans Nicox pour valoriser mon patrimoine et parce que le projet semblait sympa et attrayant, pas pour que l'on m'explique in fine pourquoi cela n'a pas marché etc....
J'attends donc des dirigeants qu'ils soient professionnels et qu'ils prennent les mesures nécessaires au succés (partenariat, lobbying politique etc.......). Pas qu'ils me tondent à longueur d'AK.
Si cela doit passer par l'esprit d'équipe, l'excellence technique où je ne sais quoi, je dirai trivialement que je m'en contre fout et que je n'attends qu'une chose : des résultats tangibles. Pour le moment et cela dure maintenant depuis un moment, les résultats ne sont pas au rendez vous, ne t'en déplaise.
Les promesses par contre sont bien toujours au rendez vous.
Oui je sais Olivier tu ne trouveras pas mes propos et ma position politiquement correcte. C'est néanmoins celle que je défends et il apparaît que je ne suis pas le seul dans ce cas. c'est peut être cela vouloir le beurre....l'argent du beurre ......et la crémière non  mais sans les emmerdes  tic tac tic tac tic tac .....un matin  cdt | |
| | | | JeanCox
Nombre de messages : 1008
Age : 70
Date d'inscription : 19/12/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 21:02 | |
| Gregnorman, je te lis avec plaisir depuis très longtemps et j'ai beaucoup de respect pour ton opinion. Cependant quand tu affirmes qu'Olivier manque de sens critique et de lucidité, je ne peux pas être d'accord. De même lorsque que tu qualifies de "zéro pointé" le bilan des 2 ou 3 dernières années. Le bilan de quoi d'abord ? - Des études réalisées ? ah bon ? - Des AK ? toutes ont été sur-sousrcrites - De la sincérité de MG ? il a tjrs fait ce qu'il a annoncé Je ne vais pas énumérer tout le reste des points de désaccord. Peu importe. Le fond du problème, amha, c'est l'horizon d'investissement, comme toujours en bourse: valoriser son patrimoine, nous le voulons tous et toutes. En combien de temps ? Voilà la vraie question... Tu me sembles (relativement) pressé. C'est une saine gestion car plus on avance vite, plus c'est susceptible de grossir si tout va bien. Faut savoir faire. Cas idéal. je suis investi en bourse (sur des valeurs risquées et moins risquées) depuis environ 30 ans. J'ai pris certaines gamelles monumentales et j'ai fait aussi des "coups" mémorables. Plus de bons coups de que de gamelles sinon je serais financièrement mort ! J'ai (je pense) su rester modeste, ce qui ne veut pas dire que je ne vais pas m'impliquer à fond dans ce que je crois pertinent. NicOx me semble pertinent. Horizon 2012. Donc je reste à bord et je rame avec l'équipage et pas contre lui. Quand je monte dans un bateau, je participe ou je débarque, je ne fomente pas de mutinerie, si tu me permets l'expression. Bref, sans aucun esprit critique, nous n'avons pas la même vision des choses, ce qui ne empêche d'ailleurs pas discuter dans un esprit cordial. Bonne soirée | |
| | | | gregnorman
Nombre de messages : 440
Age : 64
Localisation : 92
Date d'inscription : 02/06/2008
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 21:03 | |
| [quote="Carlos Alonso (carlos-al)" c'est peut être cela vouloir le beurre....l'argent du beurre ......et la crémière non mais sans les emmerdes cdt[/quote] Désolé Carlos, mais je ne vois pas bien le rapport. Pour le moment le Beurre, l'argent du beurre j'ai un peu l'impression que c'est du côté du staff de Nicox qu'il faut aller chercher. Assumer ses risques ce n'est pas faire l'autruche mais au contraire garder les yeux bien ouverts et l'esprit bien critique. Pour ce qui est de l'esprit critique, je crois malheureusement que quelques uns ici en manque un peu. Avoir l'esprit critique ne veut pas dire jouer les cassandres, mais au contraire se préoccuper de la gestion de son patrimoine. Et c'est pour cela et manifester mon désaccord avec la stratégie commerciale mis en oeuvre que je voterai non le 16 juin aux résolutions que je jugerai défavorables à mes intérêts de PP (même si cela ne sert à rien) MG t'a indiqué en off que Nicox devrait être valorisée à 24 €; Cette phrase doit'elle nous servir de Mantra ?! ou au contraire pointer les incohérences qui nous ont fait diviser ce chiffre cible par 10 ? Sur la notion de risque et d'acceptation du risque, je ne pense avoir de leçon à recevoir de personne. Je me rappelle encore la bronca que j'ai soulevé quand j'ai vendu à 9.2, et que lors d'une discussion impromptue j'ai dis que de toute manière on retournerait sur le prix de l'AK. C'est vrai je me suis trompé, on est passé en dessous! Je ne me réjouis pas d'avoir eu raison en son temps, je voudrais juste que certains d'entre vous ouvrent les yeux de temps à autre. Même si nous recollons un jour les 10 voir les 20€, je considère que des erreurs de fond ont été commises sur ce dossier. Je te souhaite néanmoins un excellent week end Cordialement
Dernière édition par gregnorman le Sam 22 Mai - 23:44, édité 1 fois | |
| | | | gregnorman
Nombre de messages : 440
Age : 64
Localisation : 92
Date d'inscription : 02/06/2008
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 21:09 | |
| Jean Cox, bsr
Le fond du sujet c'est qu'une partie d'entre nous fait une confiance aveugle à MG et son staff et qu'une autre demande des comptes sur la stratégie engagée qui ne nous semble pas correspondre à nos intêrets de PP.
Effectivement mon horizon ne se situe pas à 30 ans mais plus à 2 / 3 ans. Malheureusement, les 2 / 3 ans sont en passe de se transformer en 5 / 6 ans.
Je suis engagé sur des LBO depuis maintenant plus de 10 ans (à titre personnel) et je peux te dire que les banquiers et les actionnaires ne se gênent pas pour nous remettre dans les clous quand la direction ne leur semble pas idéquate ou que les engagements pris ne sont pas tenus.
BAT | |
| | | | cambl62

Nombre de messages : 92
Age : 75
Localisation : Arras
Date d'inscription : 27/07/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 21:43 | |
| Quels sont mes intérêts de PP?
C'est clair, pour moi: que cette boîte se développe de la façon la plus saine, la plus solide et la plus pérène possible. Est-ce être aveugle que de regarder les choses par ce bout de la lorgnette? | |
| | | | JeanCox
Nombre de messages : 1008
Age : 70
Date d'inscription : 19/12/2007
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle Sam 22 Mai - 21:48 | |
| - cambl62 a écrit:
- Quels sont mes intérêts de PP?
C'est clair, pour moi: que cette boîte se développe de la façon la plus saine, la plus solide et la plus pérène possible. Est-ce être aveugle que de regarder les choses par ce bout de la lorgnette? Clair, net, concis ! 100% d'accord | |
| | | | Contenu sponsorisé
| | Sujet: Re: L'avis des experts du Naproxcinod : la polémique enfle | |
| |
| | | | | | L'avis des experts du Naproxcinod : la polémique enfle | |
|
| | Permission de ce forum: | Vous ne pouvez pas répondre aux sujets dans ce forum
| |
| |
| |